
CASE 3
Kindly provided by James Cartwright of Edinburgh Veterinary School.
History
![BSVP1[1]](http://bsvp.org/wp-content/uploads/2013/01/BSVP11.jpg)

Clinical history
A 17 year old, male neutered, Arab cross horse (Equus callabus) presented with a 2 month history of mild but progressive anorexia accompanied by weight loss and chronic, intermittent diarrhoea. Mild elevations in ALP and GGT were present; total bilirubin and fasting serum bile acids were within normal limits.
At necropsy, gross abnormalities were restricted to the liver (fig. 1) and left lung (fig. 2).
Describe the gross findings.
Give a morphological diagnosis.
Name the aetiological agent.
What are the lesions within these visceral organs? Outline their major gross and histopathological features.
Is this condition clinically significant in the horse?
Is the aetiological agent a health risk to humans?
[expand title=”Reveal Answer”]
GROSS FINDINGS
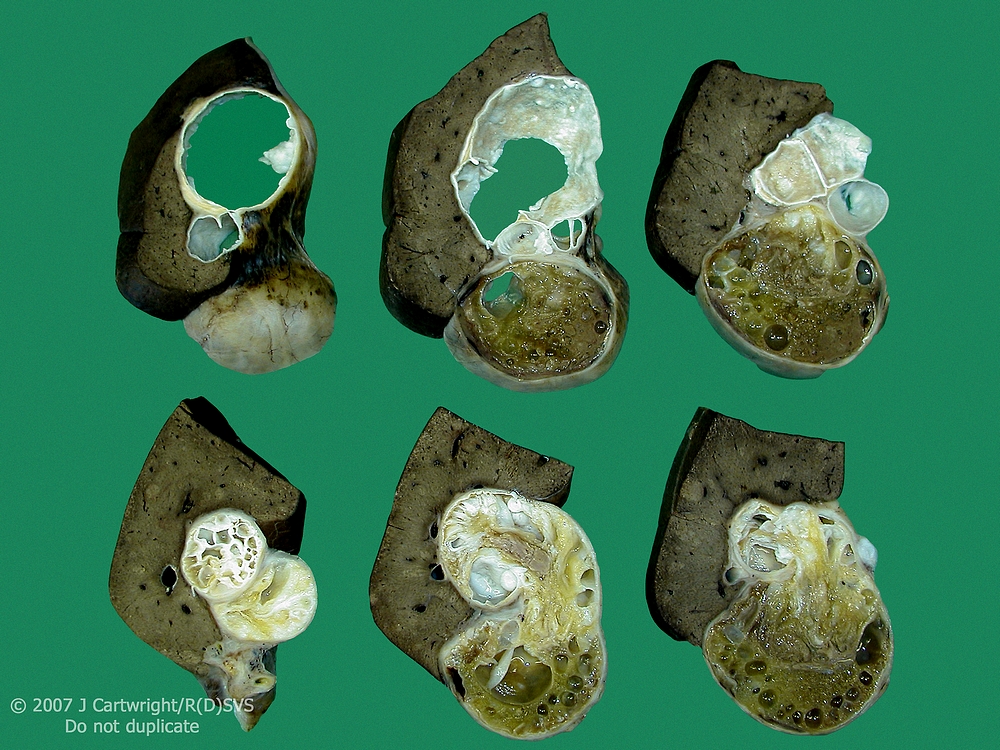
Scattered throughout the liver are numerous multifocal to coalescing, white to pale yellow/off white, roughly spherical nodules. These lesions are well demarcated and variably sized. They extend beyond the capsular surface of the diaphragmatic aspect of the liver and confer a markedly nodular appearance to the organ. A regionally extensive, white to grey reticular pattern extends over the hepatic surface.
A solitary, large, pale yellow/off white lesion is partially visible in the cranial region of the base of the left lung, close to the hilus. The lesion is roughly spherical and expansile, distorting the surface of the medial aspect of the lung.
MORPHOLOGICAL DIAGNOSIS
Cystic echinococcosis (CE), hepatic and pulmonary, horse
AETIOLOGICAL AGENT
Echinococcus granulosus
GROSS AND HISTOPATHOLOGICAL FEATURES
Ingestion of Echinococcus granulosus eggs by horses results in the slow development of CE, characterised at necropsy by the presence of numerous, variably sized, expansile metacestode stages (hydatid cysts) within visceral organs.1,2 The liver and the lungs are most frequently affected, but involvement of the kidney, spleen, central nervous system and heart may occur.3 E. granulosus typically forms roughly spherical, single-chambered unilocular cysts, although multiseptate and multilocular cysts can occur, as in this case (see illustration above).1,2,3 Protoscoleces and brood capsules form the characteristic particulate material (‘hydatid sand’) found within the metacestode.1,2
The histological appearance of the metacestode is very characteristic. The cyst wall is trilaminar, consisting of an inner, nucleated germinal layer and an outer, periodic acid Schiff (PAS) positive, acellular laminated layer; these are surrounded by a thin, host-derived fibrovascular capsule (adventitial layer).3,4 In fertile (viable) metacestodes, thickening and budding of the nucleated germinal layer produces delicate brood capsules (daughter cysts). A similar process of asexual budding within each brood capsule generates numerous invaginated protoscoleces armed with two rows of PAS positive rostellar hooks.4,5
CLINICAL SIGNIFICANCE
Equine CE is usually clinically asymptomatic; the metacestodes are well tolerated by the host and can survive for at least 16 years.1,3 Although hydatid cysts are expansile, they develop slowly and induce a minimal host response characterised by a thin adventitial layer that expands to accommodate cyst growth.3 Non-specific clinical signs, often accompanied by elevations in serum liver enzyme and bile acid concentrations, have been documented in severely affected horses and were present in this case.3,6
Nine host-adapted strains or genotypes of E. granulosus are recognised, based on morphological and biological differences within the species. Both epidemiological and genetic studies show that the horse (G4) strain is well adapted to its host and has little to no zoonotic potential.4,6
Although seven of the nine genotypes can infect humans, most cases of human CE are due to the common sheep (G1) strain. Human CE occurs globally with a sporadic to high prevalence in endemic areas. The highest prevalences are observed in communities that live in close association with both livestock (especially sheep) and dogs, and engage in suboptimal husbandry and hygiene practices.6
REFERENCES
Ronéus O, Christensson D, Nilsson N-G: The longevity of hydatid cysts in horses. Vet Parasitol 11, 149-154, 1982
Hoberg EP, Miller S, Brown MA: Echinococcus granulosus (Taeniidae) and autochthonous echinococcosis in a North American horse. J Parasitol 80, 141-144, 1994
Eckert J, Deplazes P, Craig PS, Gemmell MA, Gottstein B, Heath D, Jenkins DJ, Kamiya M, Lightowlers M: Echinococcosis in animals: clinical aspects, diagnosis and treatment. In: WHO/OIE manual on echinococcosis in humans and animals: a public health problem of global concern, eds. Eckert J, Gemmell MA, Meslin F-X, Pawlowski ZS, pp. 73-100. World Organisation for Animal Health, Paris, France, 2001
Thompson RCA, McManus DP: Aetiology: parasites and life-cycles. In: WHO/OIE manual on echinococcosis in humans and animals: a public health problem of global concern, eds. Eckert J, Gemmell MA, Meslin F-X, Pawlowski ZS, pp. 1-19. World Organisation for Animal Health, Paris, France, 2001
Thompson RCA: The development of brood capsules and protoscolices in secondary hydatid cysts of Echinococcus granulosus – a histological study. Z Parasitenk 51, 31-36, 1976
Eckert J, Deplazes P: Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Micro Rev 17, 107-135, 2004
[/expand]